FAILURE MODE AND EFFECTS ANALYSIS (FMEA)
Failure mode effects analysis (FMEA)
Also called: potential failure modes and effects analysis;
failure modes, effects and criticality analysis (FMECA)
Begun in the 1940s by the U.S. military, failure modes and
effects analysis (FMEA) is a step-by-step approach for identifying all possible
failures in a design, a manufacturing or assembly process, or a product or
service. It is a common process analysis
tool.
·
"Failure
modes" means the ways, or modes, in which something might fail.
Failures are any errors or defects, especially ones that affect the customer,
and can be potential or actual.
·
"Effects
analysis" refers to studying the consequences of those failures.
Failures are prioritized according to how serious their
consequences are, how frequently they occur, and how easily they can be
detected. The purpose of the FMEA is to take actions to eliminate or reduce
failures, starting with the highest-priority ones.
Failure modes and effects analysis also documents current
knowledge and actions about the risks of failures, for use in continuous
improvement. FMEA is used during design to prevent failures. Later it’s used
for control, before and during ongoing operation of the process. Ideally, FMEA
begins during the earliest conceptual stages of design and continues throughout
the life of the product or service.
Failure Modes and Effects Analysis Example
WHEN TO USE
FMEA
·
When a process, product, or service is being designed or
redesigned, after quality function
deployment (QFD)
·
When an existing process, product, or service is being applied
in a new way
·
Before developing control plans for a new or modified process
·
When improvement goals are planned for an existing process,
product, or service
·
When analyzing failures of an existing process, product, or
service
·
Periodically throughout the life of the process, product, or
service
FMEA
PROCEDURE
Note: This
is a general procedure. Specific details may vary with standards of your
organization or industry. Before undertaking an FMEA process, learn more about
standards and specific methods in your organization and industry through other
references and training.
1. Assemble
a cross-functional team of
people with diverse knowledge about the process, product or service, and
customer needs. Functions often included are: design, manufacturing, quality,
testing, reliability, maintenance, purchasing (and suppliers), sales, marketing
(and customers), and customer service.
2. Identify
the scope of the FMEA. Is it for concept, system, design, process, or service?
What are the boundaries? How detailed should we be? Use flowcharts to identify the scope and to
make sure every team member understands it in detail.
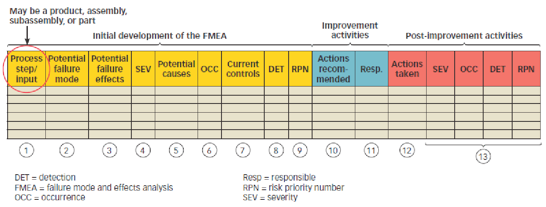
3. Fill
in the identifying information at the top of your FMEA form. (Figure 1 shows a
typical format.) The remaining steps ask for information that will go into the
columns of the form.
Figure
1: FMEA Example
4. Identify
the functions of your scope. Ask, "What is the purpose of this system,
design, process, or service? What do our customers expect it to do?" Name
it with a verb followed by a noun. Usually one will break the scope into
separate subsystems, items, parts, assemblies, or process steps and identify
the function of each.
5. For
each function, identify all the ways failure could happen. These are potential
failure modes. If necessary, go back and rewrite the function with more detail
to be sure the failure modes show a loss of that function.
6. For
each failure mode, identify all the consequences on the system, related
systems, process, related processes, product, service, customer, or
regulations. These are potential effects of failure. Ask, "What does the
customer experience because of this failure? What happens when this failure
occurs?"
7. Determine
how serious each effect is. This is the severity rating, or S. Severity is
usually rated on a scale from 1 to 10, where 1 is insignificant and 10 is
catastrophic. If a failure mode has more than one effect, write on the FMEA
table only the highest severity rating for that failure mode.
8. For
each failure mode, determine all the potential root causes. Use tools
classified as cause analysis tools, as well as the best
knowledge and experience of the team. List all possible causes for each failure
mode on the FMEA form.
9. For
each cause, determine the occurrence rating, or O. This rating estimates the
probability of failure occurring for that reason during the lifetime of your
scope. Occurrence is usually rated on a scale from 1 to 10, where 1 is
extremely unlikely and 10 is inevitable. On the FMEA table, list the occurrence
rating for each cause.
10. For
each cause, identify current process controls. These are tests, procedures or
mechanisms that you now have in place to keep failures from reaching the
customer. These controls might prevent the cause from happening, reduce the
likelihood that it will happen or detect failure after the cause has already
happened but before the customer is affected.
11. For
each control, determine the detection rating, or D. This rating estimates how
well the controls can detect either the cause or its failure mode after they
have happened but before the customer is affected. Detection is usually rated
on a scale from 1 to 10, where 1 means the control is absolutely certain to
detect the problem and 10 means the control is certain not to detect the
problem (or no control exists). On the FMEA table, list the detection rating
for each cause.
12. Optional for most industries: Ask, "Is
this failure mode associated with a critical characteristic?" (Critical
characteristics are measurements or indicators that reflect safety or
compliance with government regulations and need special controls.) If so, a
column labeled "Classification" receives a Y or N to show whether
special controls are needed. Usually, critical characteristics have a severity
of 9 or 10 and occurrence and detection ratings above 3.
13. Calculate
the risk priority number, or RPN, which equals S × O × D. Also calculate
Criticality by multiplying severity by occurrence, S × O. These numbers provide
guidance for ranking potential failures in the order they should be addressed.
14. Identify
recommended actions. These actions may be design or process changes to lower
severity or occurrence. They may be additional controls to improve detection.
Also note who is responsible for the actions and target completion dates.
15. As
actions are completed, note results and the date on the FMEA form. Also, note
new S, O, or D ratings and new RPNs.
FMEA
EXAMPLE
A bank performed a process FMEA on their ATM system. Figure 1
shows part of it: the function "dispense cash" and a few of the
failure modes for that function. The optional "Classification" column
was not used. Only the headings are shown for the rightmost (action) columns.
Notice that RPN and criticality prioritize causes differently.
According to the RPN, "machine jams" and "heavy computer network
traffic" are the first and second highest risks.
One high value for severity or occurrence times a detection
rating of 10 generates a high RPN. Criticality does not include the detection
rating, so it rates highest the only cause with medium to high values for both severity
and occurrence: "out of cash." The team should use their experience
and judgment to determine appropriate priorities for action.
Comments
Post a Comment